
Research Article | DOI: https://doi.org/10.31579/2693-2156/006
1 Department of Radiology, Rajaei Cardiovascular Medical and Research center, Iran University of medical sciences, Tehran, Iran.
2 Research center for Liver diseases, Keck School of medicine, Department of Medicine, University of Southern California, Los angeles, CA, USA.
3 Department of Radiology, Johns Hopkins Hospital, Baltimore, USA.
4 Rajaei Cardiovascular Medical ad Research center, Iran University of medical sciences, Tehran, Iran.
5 Rajaei Cardiovascular Medical ad Research center, Iran University of medical sciences, Tehran, Iran.
6 Bachelor of Radiology, Rajaei Cardiovascular Medical and Research center, Iran university of medical sciences, Tehran, Iran.
7 Department of Radiology, Amiralam Hospital, Tehran University of Medical Sciences, Tehran, Iran
*Corresponding Author: Maryam Mohammadzadeh, Assistant Professor, Department of Radiology, Amiralam Hospital, Tehran University of Medical Sciences, Tehran, Iran.
Citation: Maryam Mohammadzadeh, Ali Mohammadzadeh, Layla Shojaie, Sadaf Sahraian, Shabnam Noormohamadi, et al. (2020). The Prevalence of Coronary Artery Anomalies in Children with Congenital Heart Disease. J Thoracic Disease and Cardiothoracic Surgery, 1(2); DOI:10.31579/2693-2156/006
Copyright: © 2020 Maryam Mohammadzadeh, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 June 2020 | Accepted: 01 July 2020 | Published: 06 July 2020
Keywords: coronary artery anomalies; congenital heart disease; cardiac death; CTA; Iran
Background and purposes: Coronary artery anomalies (CAA), although rare in the general population, are common in patients with congenital heart disease (CHD). CAA can be the cause of sudden cardiac death; thus, the childhood diagnosis of CAA is essential in patients suffering from CHD. The present study aimed to investigate the prevalence of CAAs in pediatric patients with CHD in Iran.
Materials and Methods: We recruited children with CHD (one day to 21 years old), who were referred to the CT Department of Shahid Rajaei Hospital (Tehran, Iran) to undergo CT angiography (CTA) for various reasons between 2011 and 2013. We recorded age, gender, and underlying heart diseases, as well as the CTA findings, reported by a radiologist and a cardiologist. We classified CAAs using the most commonly used classification of CAA based on anatomical considerations.
Results: Among a total of 219 patients with CHD, 112 (51.1%) were male, and 107 (48.9%) were female with the mean age of 3.5 ± 2.4 years. The prevalence of CAAs was 8.7% (19 patients) with no significant difference based on gender (P-value >0.05). All 19 patients had CAAs of origin; the most common CAAs were anomalous origin of right coronary artery (RCA) from left sinus (31.6%) and anomalous origin of left main coronary artery (LMCA) from pulmonary artery (ALCAPA) (21.0%), respectively.
Conclusion: We observed a high prevalence of CAA in children with CHD, which emphasizes the importance of raising awareness about CAAs and improving the screening methods in the pediatric population suffering from CHD.
The anatomical arrangement of coronary arteries are well established and understanding the variations and anomalies has become a critical element in the evaluation of heart diseases [1]. Although coronary artery anomalies (CAA) seem to be rare in the general adult population, they are potentially life-threatening and may lead to morbidity and mortality [2]. On the other hand, CAAs are common in patients with congenital heart disease (CHD) [3]. The annual incidence of CHD is reported to be 1.35 million newborns worldwide with the highest prevalence in Asia (9.3 per 1000 live births) [4].
It is suggested for adult patients with CHD to undergo a screening coronary angiography due to the high incidence of CAAs [5]. Furthermore, non-invasive methods have been proposed for assessment of CAAs in patients with CHD, including multi-detector contrast-enhanced computed tomography angiography (CTA), magnetic resonance angiography (MRA), and ECG-gated multislice spiral CT [6-8].
Despite various imaging techniques, a large proportion of adult patients with CHD do not receive appropriate medical care, even after undergoing heart surgery in childhood [9]. Thus, considering pediatric patients with CHD is of great importance, specifically since some types of CAA are associated with a high mortality rate [10]. Conditions affecting coronary arteries include: 1) CAA associated with congenital heart conditions [Tetralogy of Fallot (TOF), transposition of great arteries, pulmonary atresia, aortic coarctation, and cyanotic congenital heart disease]; 2) CAA associated with connective tissue disease (syndromal disorders, vasculopathies, connective tissue diseases, and Kawasaki disease); and 3) Degenerative coronary artery disease [10].
Overall, the prevalence of CAAs in patients with CHD is various in different studies and ranges from approximately 11% to 14% of cases [11-13]. However, it has scarcely been evaluated in children with CHD. Tangcharoen et al. accessed the prevalence of CAAs in pediatric patients with CHD using MRA [14]; however, CTA seems to be more accurate and less costly than other imaging techniques [6,8]. Therefore, in the present study, we sought to investigate the prevalence of different types of CAA in the pediatric population with CHD who underwent CTA in a referral heart center, Tehran, Iran.
Study design
In the present cross-sectional study, we recruited children with CHD, who were referred to the CT Department of c. The study protocol was approved by Iran University of Medical Sciences, and the patients were enrolled in the study after obtaining informed consent from their parents.
The inclusion criteria consisted of pediatric patients, aged 1 day to 21 years old, who were diagnosed with CHD, based on Nada’s criteria [15], and were referred to the CT Department of Shahid Rajaei Hospital (Tehran, Iran) to undergo CTA for various reasons, including cyanosis, heart failure, systolic or diastolic murmurs, abnormal electrocardiography (EKG), abnormal chest X-ray, and abnormal blood pressure. Any patient who had a contraindication for CTA (e.g., sensitivity to contrast injection) or any patient with a history of cardiac surgery was excluded from the study.
Demographic characteristics of patients, including age, gender, and underlying heart diseases were recorded. The CTA device used in the present study was 64 slices CT unit, Siemens Healthcare, Forchheim, Germany.
The non-ionic contrast agent was injected at a rate of 5 ml/Sec after bolus sedation. Dual contrast injection was performed followed by normal saline injection and images were obtained during the diastolic phase. The CTA images were reconstructed using multi planar reconstruction (MPR) and maximum intensity projection (MIP) post-processing procedures. The CTAs were reported by a cardiac radiologist with 3 years of experience (AM) and a cardiologist with 2 years of experience.
We classified CAAs utilizing the most commonly used classification of CAA based purely on anatomical considerations in 3 categories: (1) anomalies of origin and course, (2) anomalies of intrinsic coronary artery anatomy, and (3) anomalies of termination [16].
Ethical considerations
The protocol of the study was approved by the ethics committee of Iran University of Medical Sciences. Design and objectives of the study were explained to the parents and written informed consent was obtained from those who were willing to participate in the study and they were ensured that their information will be kept confidential and analyzed anonymously. All ethical considerations of Helsinki declaration17 were met throughout the study.
Statistical analysis
Results were presented as the mean ±standard deviation (SD) for quantitative variables and were summarized by frequency (percentage) for categorical variables. Categorical variables were compared using the Chi-square test. For the statistical analysis, the statistical software SPSS version 20.0 (SPSS Inc., Chicago, IL) was used. P-values of 0.05 or less were considered statistically significant.
Overall, 219 patients suffering from CHD were referred to the CT Department of Shahid Rajaei Hospital (Tehran, Iran) to undergo CTA in the study period. 112 (51.1%) were male and 107 (48.9%) were female with the mean age of 3.5± 2.4 years and most patients (61.2%) were in the first year of life.
Among all patients, 19 (8.7%) had one or more CAAs, more than half of which (52.6%) were patients younger than two years old. There were no significant differences in the prevalence of anomalies based on gender (P >0.05). Underlying CHD included Tetralogy of Fallot (TOF), Atrial Septal Defect (ASD), and Ventricular Septal Defect (VSD).
CAAs were classified into three major groups according to origin, course, or termination (Table 1). All 19 patients had CAAs of origin including: coronary arteries with anomalous origin from aorta (68.4%; 13 patients), coronary arteries with anomalous origin from pulmonary artery (26.3%; 5 patients), and single coronary artery arising from aorta (5.3%; 1patient).
Overall, the most common CAAs were respectively anomalous origin of left main coronary artery (LMCA) and right coronary artery (RCA) from left sinus with 6 patients (31.6%) and anomalous origin of LMCA from the pulmonary artery (ALCAPA) with 4 patients (21.0%). Coronary artery anomaly (CAA) characteristics of patients with CHD who underwent CTA in Shahid Rajaei Hospital (Tehran, Iran), 2011-2013 are presented in Table 1.

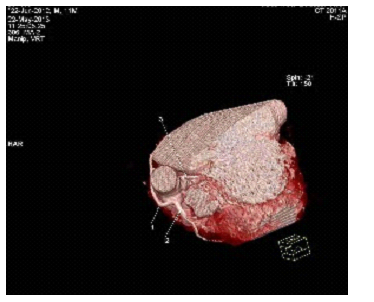
Example of Anomalous origin of coronary artery from inappropriate sinus is shown in Figure 1.
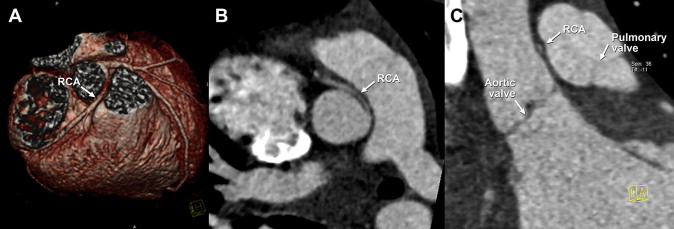
Left main coronary artery (LMCA) and right coronary artery (RCA) from left sinus of Valsalva with interarterial course. A 14-year-old boy having presyncope episodes after exercise and abnormal stress test. A) Volume-rendered 3-dimensional image displaying anomalous origin of RCA from the left sinus with interarterial course. B) Multiplanar-reformatted image in oblique axial view presents acute take-off of the RCA from the aorta. C) Multiplanar-reformatted image in oblique coronal view displays slit-like opening of the RCA, indicative of possible intramural course. Coronary CT angiography performed utilizing prospective electrocardiogram-triggered high-pitch spiral acquisition (Somatom Definition FLASH; Siemens Healthcare, Forchheim, Germany) with a calculated radiation dose of 0.3 mSv [28].
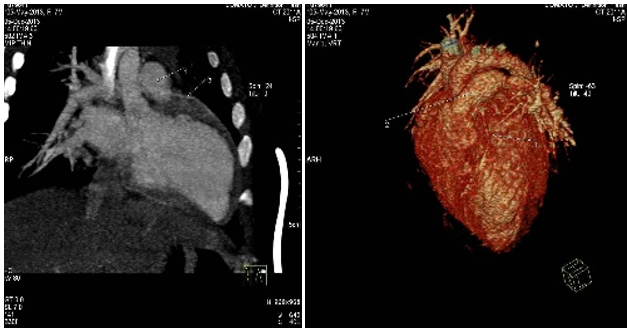
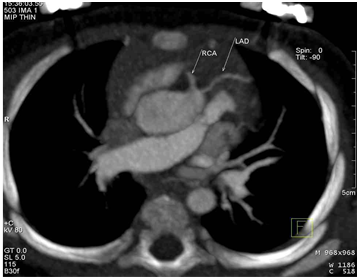
In figure 2 and figure 3; anomalous left coronary artery originating from pulmonary artery (ALCAPA) is illustrated.

A 1-year-old infant with episodic nighttime diaphoretic spells and severe systolic failure on echocardiogram referred for coronary evaluation. A) Maximum intensity projection image displaying left anterior descending artery (LAD) originating from pulmonary artery (PA). B) 4-chamber view displaying significant left ventricular chamber enlargement.
7-month old girl with left coronary artery system arising from pulmonary artery (ALCAPA). Right coronary artery arising from right sinus Valsalva and normal course. Aortic arch is left sided with normal supra aortic branch. No COA> pulmonary artery shows enlargement due to increased PAP. In the left figure, 1-LAD, 2-Pulmonary artery. In the right figure, 1-Pulmonary artery, 2-LAD.
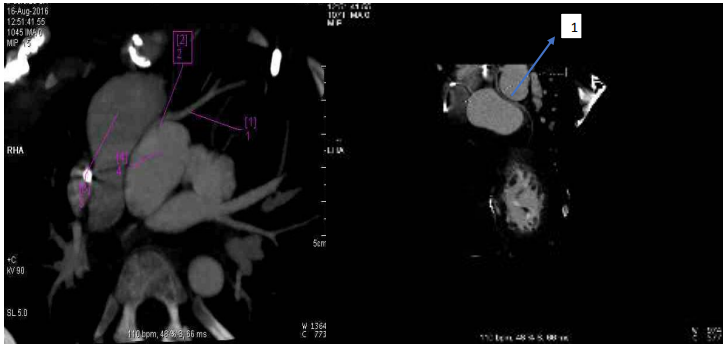
5-year old girl patient with close proximity of LAD ostium from main pulmonary artery is seen but seems originated from left coronary cusp with patent LAD. RCA is originated from right cusp and patent. Anomalous origin of LCX from RCA with retro aortic course between aorta and LA is visible. In right figure, 1-LAD, 2-Left cusp, 3-Pulmonary artery, 4-Aorta, in left figure 1-LCX from RCA.
Figure 4, is an example of anomalous origin of LAD.
10-month old boy with anomalous origin of LAD from right coronary cusp with separate ostium from RCA with prepulmonic course is seen, which needs confirmation with conventional angiography small vertical type PDA (1.5mm) is seen.
Figure 5 displays
Anomalous origin of LCX from RCA and close proximity of LAD from pulmonary artery.
Example of anomalous coronary arteries, left main and LAD arising from left coronary cusp in a
child with history of D-TGA, PA banding and septectomy is also shown in Figure 6.
11-month old boy with a history of D-TGA, PA banding and septectomy. Closed contact between RV and sternum at the level of lowest part of sternal suture. Large SAD measuring 22mm. Anomalous coronary arteries as: left main and LAD arising from left coronary cusp. RCA arising from LM and course anterior to aorta. LCX arising from posterior coronary cusp is seen into the left AV groove. Pulmonary artery shows enlargement and measuring 26mm after the banding region. Aortic arch is left sided. Very small PAD measuring 1.5 mm. 1-RCA, 2-LAD, 3-LCX.
In the present study, the prevalence of one or more CAAs was 8.7% (19 patients) in the study population, more than half of which (52.6%) were observed in patients younger than two years old. Various studies have evaluated the CAAs in general population, each using a different imaging technique and have suggested that CAAs are generally compatible with a normal life, except malignant CAAs (i.e. anomalous origination of a coronary artery from the opposite sinus (ACAOS)), which are usually asymptomatic and missed by routine examinations, such as electrocardiography, and may cause sudden death, especially in athletes and military personnel [18]. The frequency of ACAOS was 68.4% in the present study; the significant prevalence of ACAOS indicates the importance of early diagnosis of this class of CAAs; especially in patients with CHD, who have a higher risk of CAAs (11-13%) compared to the general population (1-5%) [2,18].
Furthermore, anomalous origin of LCA from pulmonary artery (ALCAPA) which was the second most common CAA in this study, is proven to be responsible for various cardiac complications, including myocardial ischemia, volume overload, ischemic cardiomyopathy, aortic valve disease, and increased risk of fixed coronary atherosclerotic disease [18]; thus, a great attention needs to be paid to this anomaly. Overall, anomalies of the main coronary arteries are established as the most common CAAs in general population [19], which is consistent with the results of the present study.
Studies suggest that from adult patients with CHD who underwent selective angiography one-third were diagnosed with CAA, while 69% of them had a clinical indication for angiography. In a British epidemiologic study by Koifman et al., the total prevalence of CAA was 11% in adults with CHD5, while in our study it was 8.7% in pediatrics with CHD. As far as review studies have indicated, the geographical distribution makes a variance in the prevalence of CAAs [4], which might justify such difference, in addition to the fact that the study population in the present study was children with CHD.
Overall, few studies have addressed the CAAs in the pediatric population with CHD. Chen et al. measured the coronary artery diameter of 145 children (aged 2 months to 11 years), and observed no gender difference regarding coronary artery diameter [20]; likewise, in the present study, the anomalies did not differ by gender, although in another study, the prevalence of CAAs was higher among adult women compared to men in general population [21]. Another Iranian study on 369 children with TOF (same center as the present study) indicated a rate of 6.8% for CAAs [22], which is consistent with the prevalence of CAAs reported in our results. Generally, the prevalence of CAAs is reported to be 0.2-0.9% in children [23,24] and 1-5% in adult population [2,18]. However, according to our study it was higher in pediatric patients with CHD (8.7%), which highlights the necessity of paying more attention to appropriate diagnosis of CAAs in these population of patients.
A few studies have elaborated the different imaging techniques for detection of CAA in patients with CHD, mainly focusing on adults. Taylor et al. compared the results of X-ray with respiratory-gated MRA on 25 adults with CHD and suggested the use of the combination of these two methods for CHD patients, but reported some limitations for each technique [25] Similar to our study, Goo et al. have also suggested CTA as an appropriate diagnostic imaging tool in CHD patients [26]. In a later study also directed by Goo et al. it was concluded that preoperative cardiac CT might be beneficial in recognizing coronary artery anatomy in infants with tetralogy of Fallot [27].
Extensive number of review studies have also determined that CTA provides sufficiently accurate anatomical information in difficult-to-image patient groups [6,8].
The present study had some limitations including the missed cases which arose from the inconvenience of children to undergo CTA, and lack of cooperation to hold their breath for 10 seconds, which are the problems of most imaging studies on the pediatric population. In addition, the results of CTA, obtained in the present study, were not compared with other modalities or gold standard methods to estimate the diagnostic accuracy of CTA, which were beyond the objectives of the present study. Future studies should evaluate the specificity and sensitivity of different modalities for finding CAAs in children with CHD.
In this study, the prevalence of CAA in children with CHD was 8.7%, more than half of which were younger than two years old. Given the prevalence in young children, further studies can be enormously helpful for the future. Some common types of CAA are associated with a high mortality rate and may cause sudden death, especially in athletes. Therefore, it is essential to raise awareness about CAAs and improve the screening methods in the pediatric population suffering from CHD. It is strongly suggested that radiologists and cardiologists work as a team to achieve a more accurate interpretation of the CTAs further to decrease the mortality and morbidity of this condition.
There is no conflict of interest regarding the manuscript. There is no financial relationship with the organization that sponsored this research and we have full control of all primary data and it is available for review upon request.
No funding source was applicable for this research.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
